By Carole Youakim, Pulmonary and Allergy Specialist
Asthma is a major public health problem with a huge social and economic burden affecting 300 million people worldwide. Infection with respiratory viruses; including Rhinovirus, Influenza Virus and Respiratory Syncytial Virus; is the major cause of common cold. Influenza is the most common infection during the winter months, frequently reaching local or national epidemic proportions. Viral respiratory infections frequently trigger asthma exacerbations in children and adults and may contribute to asthma morbidity and mortality. In fact, up to 80% of asthmatic children have intermittent wheezing after viral infections and 70% of asthma exacerbations in adults are attributed to respiratory viral infections. Viral infection and allergy interact to increase the risk of exacerbation. One study reported that allergen sensitization, exposure to sensitizing allergen, and respiratory tract viral infection, acted in a synergistic manner to significantly increase the risk of hospitalization with acute asthma.
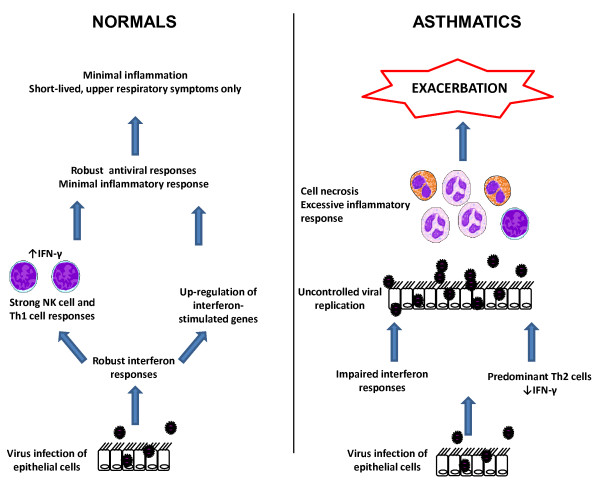
Several mechanisms for the viral-induced exacerbation of asthma have been reported. Recent evidence points to impaired innate interferon responses in the airway of asthmatic subjects as a risk factor for asthma exacerbations. Viral replication is increased in cells from asthmatics compared to non asthmatic subjects and impaired interferon and TH1 responses results in uncontrolled viral replication and an exaggerated inflammatory response. Seasonal influenza vaccination in asthmatic patients is strongly recommended.
Several studies have demonstrated that inhaled corticosteroids (ICS) reduce the release of inflammatory mediators from airway epithelial cells infected with viruses and the combination of inhaled steroids and long acting ß2 agonists (LABA) have additive or synergistic effects. Leukotriene receptor antagonists (LTRA) can prevent common cold-like symptoms and suppress inflammation following viral infections and it seems that combined use of ICS and LTRA may be more useful than use of either drug alone.
References : J Allergy Clin Immunol 2011;128:1165-74 / Lancet 2010;376:826-834 / Curr Opin Allergy Clin Immunol 2012;12(2):151-157 / BMC Medicine 2012;10:27 / PLoS ONE 6(11): e27898. doi:10.1371/journal.pone.0027898 / Allergology International 2007;56:263-267.